The Assumption about Physical Intervention Training
WHAT DO YOU DO?
This seems to be an innocent question with a straight forward answer. However, when asked by someone who works in healthcare industry, assumptions take over and most people are convinced they know exactly what that entails – lets look at the options
I AM A D.ESCAL8™ TRAINER
Well frankly no one understands that yet – I believe this may be the answer for the all rounder however we need to proceed to more common options.
I DELIVER PHYSICAL INTERVENTION TRAINING
This leads to a response that is usually underpinned by the phrase – “restraint training”
This is not the case, I do not teach restraint in the manner that they perceive. Most say oh yes I have done that or comment about floor restraint. In actuality I do teach some restraint however the physical skills I teach are very different to your perception of the concept. In my experience most people who experience D.ESCAL8 having been on other training are astounded.
One individual last week fed back that I had taught him restraint. I was wary as he seemed an intelligent person, therefore I chose not to respond to give him more space to explain.
"you taught me to restrain myself from my desire to intervene"
On hearing this I knew he had got the point and was using the word for himself. He had done another course in the last 6 weeks that should have been very similar but according to him had no where near the same focus.
In that moment, after his initial comment, when I chose to let him talk further – I restrained myself too.
Over the years I have taught hundreds of people who say during the training course introduction that they have done this sort of training before, a lot are quite arrogant that they do not need to be on the course due to having done this before. ALL have reported that what D.ESCAL8 does is incredibly different and notably better than any previous training experience.
The problem with getting into the physical conversation is people assume you to be a martial artist or a bouncer rather than the all round D.ESCAL8 trainer.
Is the focus to get staff confident in achieving success in the skills – well yes. However that is secondary to the real focus – to be so good at the skills you never need to use them..
What do you mean? I hear you say. Well another option.
I DELIVER IMPROVEMENT IN STAFF CONFIDENCE, ACCEPTANCE AND RESILIENCE THROUGH BUILDING RELATIONSHIPS AND COMPASSION WITH THOSE INDIVIDUALS WHO ARE IN DISTRESS
OK most people have fallen asleep before I finish that one – however I think it is closer to what I actually do. One of the issues with this one is the fact that some people actually want physical intervention and think I am just a psychologist, not capable of the high level of physical skill, rather than an well rounded D.ESCAL8 trainer.
And so an in reality you need to have the physical skill level to give you the confidence to remain open in the situation and not reacting due to fear and inexperience.
The truth is I am both, I have developed a system that delivers the skill level to achieve the desired result, AND the psychologist in me has developed a focus to reduce the likelihood of using any physical skill at all.
While I see this as the best of both worlds, normal people fall into making one or other assumption about what I do and therefore assume they understand the D.ESCAL8™ concept.
Teaching the staff to manage their emotion helps their work relationships & I know I can help alter staff members to maintain an open heart and the confidence to have an empty mind when dealing with those in distress.
This leads to less conflict and better relationships.
Better relationships leads to reduction in levels of distress for all parties.
Get in touch to discover how we can reduce interventions and develop healthy relationships in your service
Challenging Behaviour is a term the healthcare sector has misused for years. When the term was originally introduced, it was an attempt to move away from the then widely used term "behaviourally disturbed". The healthcare sector recognised that the term had become associated with some very negative connotations and therefore should not, in good conscience, be given to an individual.
A service director the other day commented how it was only on Physical Intervention training that the staff start questioning to the Nth degree about scenarios and possible outcomes of events. She stated that it would not happen on a first aid course. Well I know a first aid trainer who would disagree, however I have been on a lot of training as a participant in the last year (see biog) and can agree her point is valid.
From Inception D8 was formed as a method of getting high quality training to those who care for individuals in distress. Part of that concept involves smaller companies and individuals who find accessing training prohibitive for various reasons. Apart from the obvious cost implications with running a full training course there are also the implications regarding closing a business to release staff for the course to occur.
When under pressure we respond in a small number of differing ways. These tend to be in 2 main camps. Those who feel the need to control and those who have a more relaxed attitude. The question is which has a better effect on the person in distress? Picture this, you are under pressure and in distress and you shout at your partner "just get me my dinner!" and your partner replies "No, you will not talk to me in that manner! ENOUGH now."
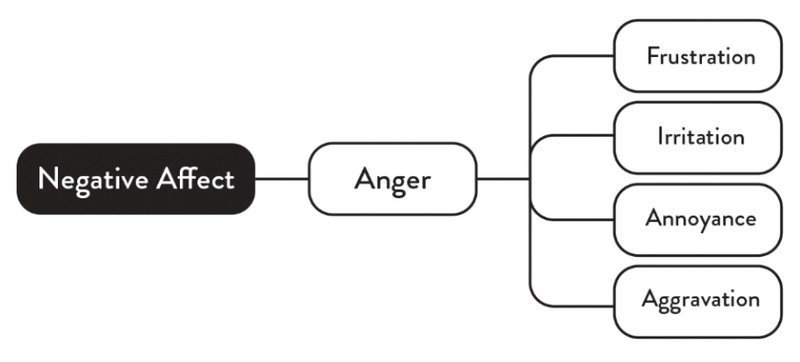
Over the last few years we have had a terrific response in terms of de-escalation with our course incorporating Affect Labelling. Emotions arise to make us pay attention to our environment. The more emotional our experience, the less we can think clearly, resist impulses, and engage in constructive problem-solving. By creating even the simplest label, we learn to express what we are experiencing. At a rudimentary level, we think about what is causing us to feel emotion and take action to experience either more or less of the emotion, depending on the situation.
The mind shift almost always travels from introductions where people say / imply things that contradict the basic philosophy of the course to an ending where people state publicly (or privately to me) how they always thought like this. Usually adding something like - “it is great that a training like this exists so that all those other people I work with whose attitude needs adjusting can access it”.
The Assumption about Physical Intervention Training
What would you do? This seems to be an innocent question with a straight forward answer. However, when asked by someone who works in healthcare industry, assumptions take over and most people are convinced they know exactly what that entails – lets look at the options
The term debriefing is an industry-used term. In our industry while useful it is often misunderstood when talking about application at ground floor or grassroots level. When discussing the term de-briefing we @de-escalate.com have separated the term debriefing into different areas. I will discuss one of these here.
If there is any indication or suspicion that anyone has suffered an injury or psychological trauma following the incident / use of physical intervention they must receive treatment and support as soon as is reasonably possible. Debriefing is misused as a term, and while analysis is important in a Positive Behaviour Support framework, your D.ESCAL8™ facilitator discussed these two areas and the differences between debriefing and offloading.
Teaching different groups can lead to predictable responses. When you teach a group where half the participants work with younger kids (under 11 ish) and the other half work with young people (teens) there is a clear dichotomy in their attitudes and responses around problem behaviour. It all comes back to the issue around the distractor versus the reinforcer.
I have wanted to do a post about Hanlon's Razor for a while and the mask issue has led to me combining that here. Our non verbal communication being misinterpreted or misunderstood should not be considered intentional.
This is a series of images sent to me by the area boss. It's not merely about the evaluations people provide at the end. It’s about the deeper consolidation achieved through meaningful conversations within the team. These conversations foster understanding, collaboration, and alignment, which are far more impactful than numerical scores or rankings. The true value lies in engaging dialogue that strengthens bonds and resolves challenges. Success stems from shared insights and collective growth within the team. Conversations truly matter in building trust and unity.